The enigma surrounding coffee-colored serum
Dr. Sailuja Maharjan, Dr. Sristi Upadhyay, Dr. Srinivas Chakravarthy
Dr. Sailuja Maharjan1 , Dr. Sristi Upadhyay 2 , Dr. Srinivas Chakravarthy3
1Department of Pathology, Kulhudhuffushi Regional Hospital, Kulhudhuffushi, Maldives
2Department of Pediatrics, Kulhudhuffushi Regional Hospital, Kulhudhuffushi, Maldives
3Department of Laboratory Medicine, Kauvery Hospital, Chennai, India
Corresponding Author:
Dr. Sailuja Maharjan,
Kulhudhuffushi Regional Hospital,
Kulhudhuffushi, Maldives.
Email: sailuzaa73@gmail.com
APFCB News Volume 4, Issue 1
Introduction
Visual inspection of the serum sample can give valuable information regarding the underlying condition of the patient. The most commonly observed visual discoloration of serum after centrifugation of the sample are red, icteric or milky appearance. (1) These have the potential to interfere with the biochemical assays and may lead to erroneous interpretation. However, modern automated analyzers are able to quantify hemolysis, icterus and lipemia (HIL) interference more accurately than the traditional visual inspection of the sample, thereby improving the quality and efficiency of the laboratory analysis. (2,3) Nevertheless, the visual inspection of the serum sample still provides some clues when there is unusual serum discoloration. (4) Herein we report a patient with coffee colored serum as an adverse effect of eltrombopag. Therefore, we alert the laboratory professionals and highlight the importance of visual inspection of the serum sample in a clinical laboratory and explore the possibilities. Furthermore, eltrombopag at high dose (200mg) can interfere with bilirubin assay based on the methodology used in the detection systems.
Case Report
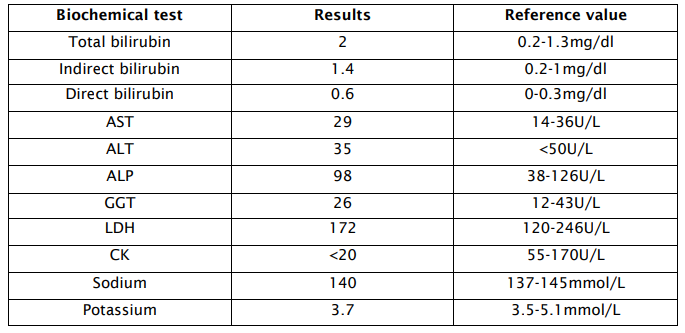
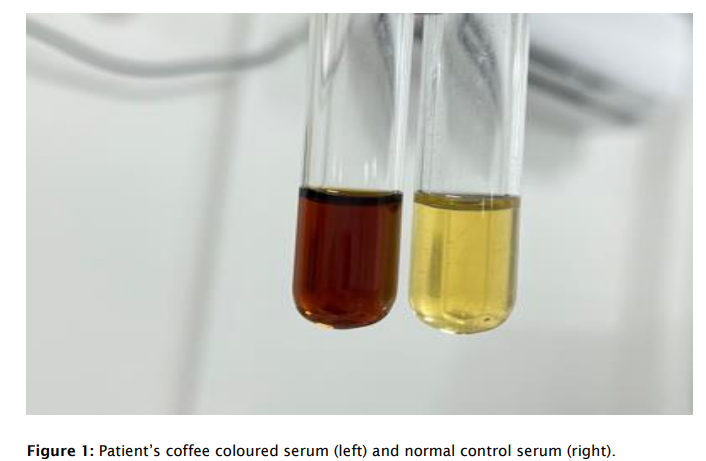
We report a case of 15-year-old female who was presented with complaints of cough for one month.She had consulted at a higher centre where bronchoalveolar lavage was done and the aspirate showedgrowth of Pseudomonas colonies on culture sensitivity testing. She was admitted in our hospital for intravenousantibiotics. History was notable for allogenic peripheral stem cell transplant done 9 years back for beta thalassemia major, complicated by graft versus host disease and recurrent pulmonary infection. She was transfusion dependent as there was persistent anemia and thrombocytopenia. The patient was under erythropoietin as well as eltrombopag 100mg since February 2024, which has been increased to 200mg since past 2 months. Her blood sample was received in our laboratory for a complete blood count and biochemical tests. After centrifugation of the sample, the serum showed an unusual color of coffee brown(Figure 1). On analyzing the sample further with VITROS 5600 analyzer, the HIL index was <15, 5 and <20 respectively (Package insert limit of HIL: <15, <2, <20 respectively). The biochemical test results are shown in table 1. According to the literature, the possible causes of the brownish color serum could be related to methemoglobin, metalbumin, hemolysis or myoglobin. We discussed the abnormal serum color with the clinician and ruled out methemoglobinemia clinically as oximetry was maintained at 95% and there was no cyanosis, dizziness or SOB. Furthermore, we added LDH, which was normal and helped in excluding hemolysis. Additionally, CK was normal, which ruled out rhabdomyolysis. Urinalysis was within the normal limit with negative hemoglobin or myoglobin. After excluding all possibilities, we started exploring if any medication could lead to coffee-colored serum. We noted a very handful of cases reported in the literature with brown serum in patients under eltrombopag therapy. Therefore, we concluded that the coffee-colored serum in our patient was due to eltrombopag after ruling out other possibilities. Furthermore, we noted drug interference with bilirubin as the total bilirubin of the patient’spre and post increment of the dose of eltrombopag was 0.4mg/dl and 2mg/dl respectively
Discussion
Brownish discoloration of serum may be caused due to methemoglobin, hemolysis, methalbuminemia or Myoglobin. (1) Methemoglobinemia occurs when iron in hemoglobin is oxidized from ferrous state to ferric state, compromising the release of oxygen to tissues. It can be genetic or acquired when the patient is exposed to certain drugs like dapsone, local anesthetics, nitrates, quinones or some chemicals like chlorates. (5) Methemoglobinemia can be excluded by arterial blood gas analysis and co-oximetry. (6) Laboratory findings in in-vivo hemolysis include low haptoglobin, indirect hyperbilirubinemia and elevated LDH.4Serum estimation of myoglobin or CK should be performed to rule out rhabdomyolysis in proper clinical context.5
Some drugs are very notorious for abnormal discoloration of body fluids like urine or serum. Another rare cause of brownish colored serum is due to adverse drug effects of eltrombopag. Eltrombopag is an oral thrombopoietin receptor agonist approved for the treatment of immune thrombocytopenia, severe aplastic anemia and thrombocytopenia associated with Hepatitis C infection. (3,4,7) It is a brownish to yellowish powder which exhibits pH dependent change in color. (8,9) The patients with high dose of the drug (150mg per day) are found to have adverse drug reaction like abnormal serum coloration or skin hyperpigmentation. (3,4,8,10) Cardamone et al. have reported the interference of high dose eltrombopag or its metabolites with certain analytes like bilirubin in spectrophotometric assays. (7) Additionally, eltrombopag is a hepatotoxic drug and can cause challenges in assessment of hyperbilirubinemia based on the methodology used. (3,4,9) Therefore, it is imperative to distinguish between true hyperbilirubinemia and drug induced pseudohyperbilirubinemia for accurate interpretation of the results. (7) This can be achieved by comparing the pretreatment and posttreatment bilirubin in absence of clinical feature of hepatotoxicity or normal liver enzymes. In our case, the increment in bilirubin could possibly be attributed to drug interference at high doses. Similarly, Fuentes et al. reported that a high dose of eltrombopag can positively interfere with bilirubin on the VITROS 5600 automated detection system. (3) The possible analytical interference of this drug should be recognized by the lab professionals as they are methodology dependentand this information should be shared with the clinicians.
Conclusion
Visual inspection of plasma is crucial in laboratories as abnormal colored plasma requires special attention. Though eltrombopag is not a commonly encountered drug in clinical practice, its adverse pharmacologic effect should be kept in mind by laboratory professionals. Additionally, comparing pre and post treatment bilirubin in patients under eltrombopag can help in monitoring hepatobiliary function to ensure accurate interpretation of the results.
Patient consent for publication: obtained
conflict of interest: none
1. Dukic L, Maric N, Simundic AM. Dark brown serum and plasma samples: a case report. Biochem Med (Zagreb) 2020;30(2):021002.
2. Farell CJ, Carter AC. Serum indices: managing assay interference. Annals of clinical biochemistry. 2016;53. 527-38.
3. Poventud-Fuentes I, Garnett E, Despotovic J, Devaraj S. Interference of eltrombopag with bilirubin measurements on the Vitros 5600 analyzer. J Clin Lab Anal. 2021 Aug;35(8):e23796
4. Rojas CR, Santamaria CJ, Belda ODP, Noguero EM. Coffee Colored Serum, Adverse Reaction of Eltrombopag. The electronic Journal of the International Federation of Clinical Chemistry. 2023(34); 258-61.
5. Afzal N. A Unique Case of Dark Brown Plasma: Why Colour Variation should be Reported.JCPSP Case Rep 2023; 1:60-62.
6. Prus-CzarneckaZ, Fuezery A, Noga T, et al. BMJ Case Rep 2023;16:e252885.
7. Cardamone D, Milone MC, Glaser L, Frey NV, Kricka LJ. Eltrombopag and serum of a different hue. Arch Pathol Lab Med. 2013 Sep;137(9):1175.
8. Rodgers GM, Kurtti AL, Gilreath JA. Are eltrombopag plasma and skin hyperpigmentation related? The eyes have it. Am J Hematol. 2019;94:394–395.
9. Cheng THT, Tsui TKC, Kwok JSS, Lit LCW, Wong EYL, Kam RKT, Grote-Koska D, Staaden A, Okada H, Fuke N, Wong RSM, Li CK, Chan MHM. Comprehensive characterization and resolution of discrepant spectrophotometric bilirubin results in patients on eltrombopag therapy. Clin Chem Lab Med. 2020 Sep 25;58(10):1713-1723
10. Atay H, Kelkitli E, Turgut M. A rare side effect: eltrombopag associated hyperpigmentation. G Ital Dermatol Venereol. 2020 Dec;155(6):803-804.
